
 See
more of the story
See
more of the story
Was the Trump administration trying to play Minnesota for a sucker on health care? That's what Gov. Mark Dayton alleged last week — a claim that wasn't contradicted when Dayton announced Friday that the reinsurance waiver the state had sought from the feds had been approved.
The Trump play, as Dayton described it in a letter released Tuesday: String Minnesota along for months with the promise of federal money to help pay for a reinsurance program that would keep health insurance premium rates affordable on the state's private-insurance purchasing exchange, MNsure. Tell the poor dupes in Minnesota how to craft the program and apply for a waiver to draw down $208 million in additional federal funds. Assure them that no other federal/state health care arrangement in Minnesota would be affected.
Then just before the waiver's approval deadline, tell Minnesota that there's been a little misunderstanding. The waiver is actually going to nick the state's Basic Health Plan, a.k.a. MinnesotaCare, for a cool $369 million. With the waiver approved, the net hit on Minnesota balance sheets would be $161 million.
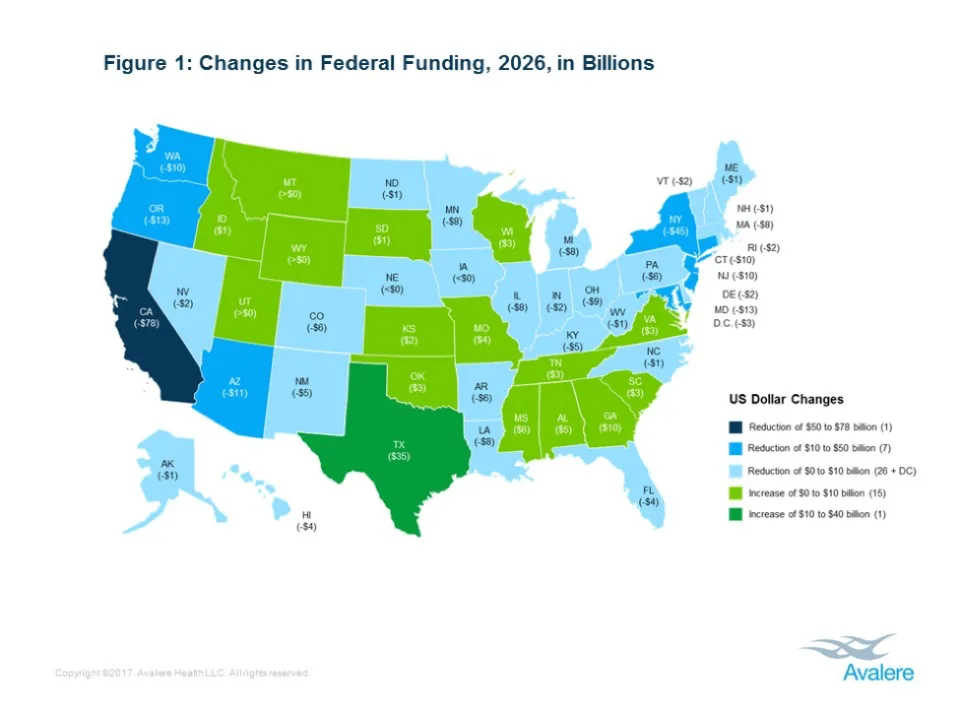
That's just for the next year. Trump and the Republicans in Congress have another kick in store after that for Minnesota and the other states that opted to provide Medicaid or their own state-sponsored affordable health insurance to the working poor. Those states would lose money bigly under the latest iteration of "repeal and replace" anti-Obamacare legislation. The bill known as Graham-Cassidy awaiting action in the U.S. Senate would deprive Minnesota of an estimated $8 billion by 2026, according to Avalere Health, a consulting firm.
Many reliably Republican states would fare better under Graham-Cassidy. Bet you're not surprised. In these latter days, it's bipartisan lawmaking — the kind that created MinnesotaCare 25 years ago — that would be surprising.
In 1992, a Republican governor and a bipartisan legislative task force set out to make health insurance affordable for Minnesota's working poor. It designed MinnesotaCare to be funded by modest income-based premiums and a state subsidy paid for with a 2 percent tax on health services — the "provider tax." At the start, very little federal money was involved.
Today, 87 percent of the government share of MinnesotaCare's funding comes from the feds. "It's a really good deal," DFL Sen. Tony Lourey told me last week.
But doesn't it make MinnesotaCare vulnerable to the "vagaries" (that's today's polite euphemism) of Washington politics? I asked.
A long pause was followed by a terse answer: "Yes."
The possibility that the federal government would become a slippery partner on health care funding seemed to come as a shock last week to state pols — particularly DFLers. A few Republicans may have muttered "I told you so." My fuzzy mental tapes include the voices of Republican legislators in 2011 warning about too much dependence on the federal government as Dayton seized the opportunity Obamacare afforded to enroll a larger share of the state's working poor in Medicaid, mostly at federal expense.
A few years later, MinnesotaCare was deemed a Basic Health Plan under the Affordable Care Act. Some Republicans called for scrapping MinnesotaCare instead. The state insurance plan for people with incomes between 133 percent and 200 percent of the federal poverty level was no longer necessary, they argued. That population could buy insurance on the MNsure exchange and qualify for tax subsidies to help pay for it.
The problem with that argument: Health insurance plans on the MNsure exchange often involve deductibles and copays too high for low-income people to afford, even with subsidies to help them pay the premiums. That's why MinnesotaCare has remained a popular health insurance option in the ACA era. A large share of its 90,000 enrollees live in greater Minnesota.
That geography ought to inspire support for the program within the disproportionately rural Republican legislative caucuses. Instead, GOP legislators scoffed at Dayton's 2017 proposal to allow people with somewhat higher incomes and/or few other health insurance options to enroll in MinnesotaCare.
The Legislature's GOP majorities have also ignored the governor's calls to continue the provider tax — MinnesotaCare's original funding source — past its scheduled sunset on Dec. 31, 2019. Yet they made that tax the primary source of funds for the reinsurance program they designed earlier this year in an effort to bring down the premiums charged by insurers on the MNsure exchange.
More than that: The provider tax has morphed into a politically convenient way for legislators in both parties to balance the state human services budget. It's become a way for legislators to have their cake — a robust Medicaid program for the very poor — and eat, er, hide a portion of its costs, keeping them off the general-fund books. This year, about $225 million from the Health Care Access Fund (the accumulated provider tax proceeds) will pay for Medicaid. Another several hundred million dollars will go to a variety of smaller items that used to be financed by the general fund.
That budgeting trick's days were numbered, even before threats to the flow of federal health care funds into this state appeared last week. With the feds apparently going soft on their commitment to helping this state keep low-income people insured, Minnesotans are going to be asking candidates for governor and the Legislature in 2018 how firm their own commitments are to that good cause.
Lori Sturdevant, an editorial writer and columnist, is at lsturdevant@startribune.com.





{kind=link}